
Mr. Oculus says,
Glaucoma + Diabetes = A Risk You Can’t Afford to Ignore
Think of your eye like a sink with the faucet on and the drain open. As long as the outflow matches the inflow, the eye pressure stays stable. In glaucoma, the drainage clogs, which causes the fluid to build up in the eye.
Glaucoma doesn’t hurt. It doesn’t blur your vision early. But it does steal sight permanently. If you have diabetes, your risk of glaucoma is 36% higher.
You can’t rely on symptoms. You can depend on annual eye exams—early detection = damage control. You may need drops, lasers, or surgery, but you need to know your numbers (especially eye pressure).
Bottom line: Sight loss from glaucoma is irreversible, but preventable. If you have diabetes, screening your eyes for glaucoma must be a part of your care plan.
Glaucoma isn’t rare. But it’s rarely caught early.
An estimated 80 million people worldwide live with glaucoma today, and the numbers are rising. But surprisingly, over half don’t know they have it.
Glaucoma causes progressive, irreversible damage to the optic nerve, and often does so without pain or early visual symptoms. That’s why it’s called the silent thief of sight.
Now here’s where things get even more serious:
If you have diabetes, your risk of developing glaucoma is significantly higher – 36% higher!
Why is glaucoma so dangerous?
Understanding what’s happening inside the eye helps one understand why glaucoma is such a threat to vision.
A quick anatomy detour
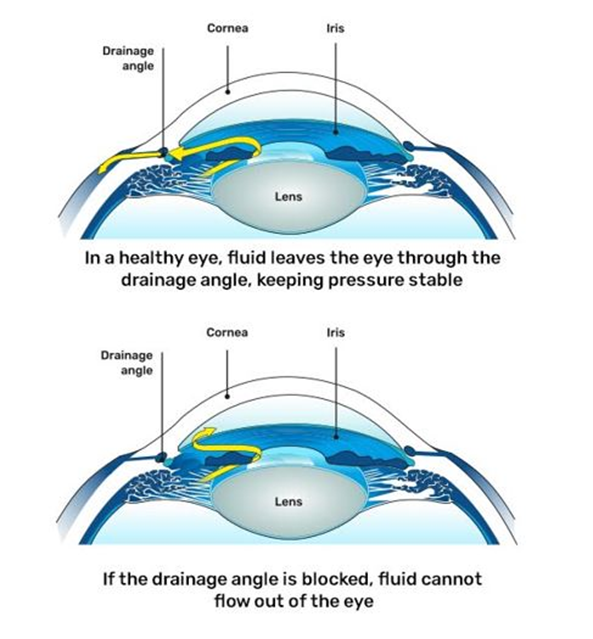
Inside the front part of the eye, there’s a clear fluid that keeps the eye healthy by nourishing it and maintaining the right pressure. The eye is always making this fluid, and it needs to drain out properly through a tiny drainage system where the colored part of the eye (the iris) meets the clear front layer (the cornea). If the fluid doesn’t drain well, it can lead to pressure build-up inside the eye.
The balance between production and drainage keeps intraocular pressure (IOP) within a healthy range, usually between 10 and 21 mmHg.
What goes wrong in glaucoma?
In glaucoma, this drainage system stops working efficiently, either because the meshwork becomes blocked, scarred, or compressed.
As a result:
- Aqueous humour builds up
- IOP (intra-ocular pressure or eye pressure) rises gradually (or suddenly, in rare cases)
- The elevated pressure damages the optic nerve
- Over time, this leads to progressive vision loss, starting from the peripheral field, meaning the outer edges of your vision, or what you see when you’re not looking directly at something.
What’s the connection between diabetes and glaucoma?
Let’s look at the mechanisms:
1.Primary Open-Angle Glaucoma (POAG)
The most common type. The drainage angle is open, but fluid drains too slowly, causing a gradual rise in eye pressure. It’s painless and usually detected during routine eye exams.
2. Chronic angle closure glaucoma- the drainage pathway is narrow in this condition, so fluid cannot drain properly. This leads to a buildup of eye pressure gradually over a period of time and causes glaucoma
3. Angle-Closure Glaucoma
A medical emergency. The drainage angle suddenly blocks, leading to a rapid spike in pressure. Symptoms include eye pain, headache, blurry vision, halos, and nausea. Requires urgent treatment.
3. Normal-Tension Glaucoma (NTG)
Damage to the optic nerve occurs despite normal eye pressure, likely due to poor blood flow. Risk increases with migraines, low blood pressure, or autoimmune disorders.
4. Secondary Glaucoma
Results from another eye condition, such as injury, inflammation, steroid use, or diabetes. Neovascular glaucoma, linked to diabetic eye disease, is especially aggressive and more challenging to control.
So what should you do?
If you have diabetes, your eyes need regular check-ups, whether or not you have symptoms. Most people don’t realise that diabetes can quietly damage the eyes in more than one way. It can lead to diabetic retinopathy, where high blood sugar harms the tiny blood vessels in the retina. It also increases your risk of glaucoma, where pressure builds up inside the eye and damages the optic nerve.
Both conditions can lead to vision loss, but can also be caught early with routine eye exams. Protecting your vision starts with knowing the risks.
Want to understand diabetic retinopathy better? Check out our detailed section on diabetic retinopathy for more information.
How does your eye doctor diagnose glaucoma?
As we said earlier, glaucoma often flies under the radar until it’s too late. That’s why your yearly eye check-up must also include a comprehensive glaucoma workup.
This includes:
| Test | Purpose |
| IOP Measurement (Tonometry) | Checks intraocular pressure |
| Optic Nerve Imaging (OCT) | Detects early structural damage |
| Visual Field Test (Perimetry) | Maps peripheral vision loss |
| Gonioscopy | Assesses drainage angle anatomy |
| Pachymetry | Measures corneal thickness, which influences IOP accuracy |
| Fundus Photography | Documents optic nerve appearance over time |
Can Glaucoma be treated?
There’s no permanent cure for glaucoma, but the good news is:
If caught early, it can be controlled, and vision can be preserved.
Treatment focuses on lowering eye pressure (IOP) to prevent further damage to the optic nerve. Here’s how that’s done:
1. Eye Drops
These drops either:
- Reduce the production of fluid inside the eye, or
- Help the fluid drain out more effectively
They’re simple to use but must be taken regularly, missing doses can lead to rising pressure again.
2. Oral Medications
Sometimes, your doctor may prescribe tablets (like carbonic anhydrase inhibitors) to lower IOP, especially in emergencies quickly or when eye drops alone aren’t enough.
3. Laser Treatment
For open-angle glaucoma, a common option is SLT (Selective Laser Trabeculoplasty).
- It helps improve fluid drainage by targeting specific cells in the drainage meshwork.
- It’s a painless, outpatient procedure that can reduce or delay the need for drops.
4. Surgery
If pressure remains high despite medications or laser:
- Your doctor may recommend trabeculectomy, a procedure that creates a new drainage pathway.
- Newer, less invasive options like MIGS (Minimally Invasive Glaucoma Surgery) are also available. They use tiny implants or devices to lower IOP and speed up recovery.
5. Treatment for Neovascular Glaucoma
In advanced diabetic eye disease, abnormal blood vessels can block the drainage angle.
This type of glaucoma is more complex to manage and often needs a combination of:
- Anti-VEGF injections (to stop abnormal vessel growth), and
- PRP (Pan retinal Photocoagulation) laser to reduce oxygen demand in the retina
These are combined with IOP-lowering drops or surgeries as needed.
Treatment plans are highly individualised. But the sooner glaucoma is detected, the more vision can be saved.
Who needs earlier or more frequent screening?
You may need 6-monthly exams (instead of annual) if:
- You’ve had diabetes for over 10 years
- Your HbA1c is persistently >8%
- You already have diabetic retinopathy
- There’s a family history of glaucoma
- You’re over 40 years old
- You’ve had episodes of optic neuritis, uveitis, or eye trauma
- You’re on chronic steroids (oral or topical)
Takeaway:
Living with diabetes already means juggling appointments, lab tests, an d lifestyle changes. Adding one more eye exam might feel like a chore.
You don’t need symptoms to take action. You need information, the right screening, and a doctor who knows what to look for. That’s what changes the story from loss to prevention.